Ayva Ortho
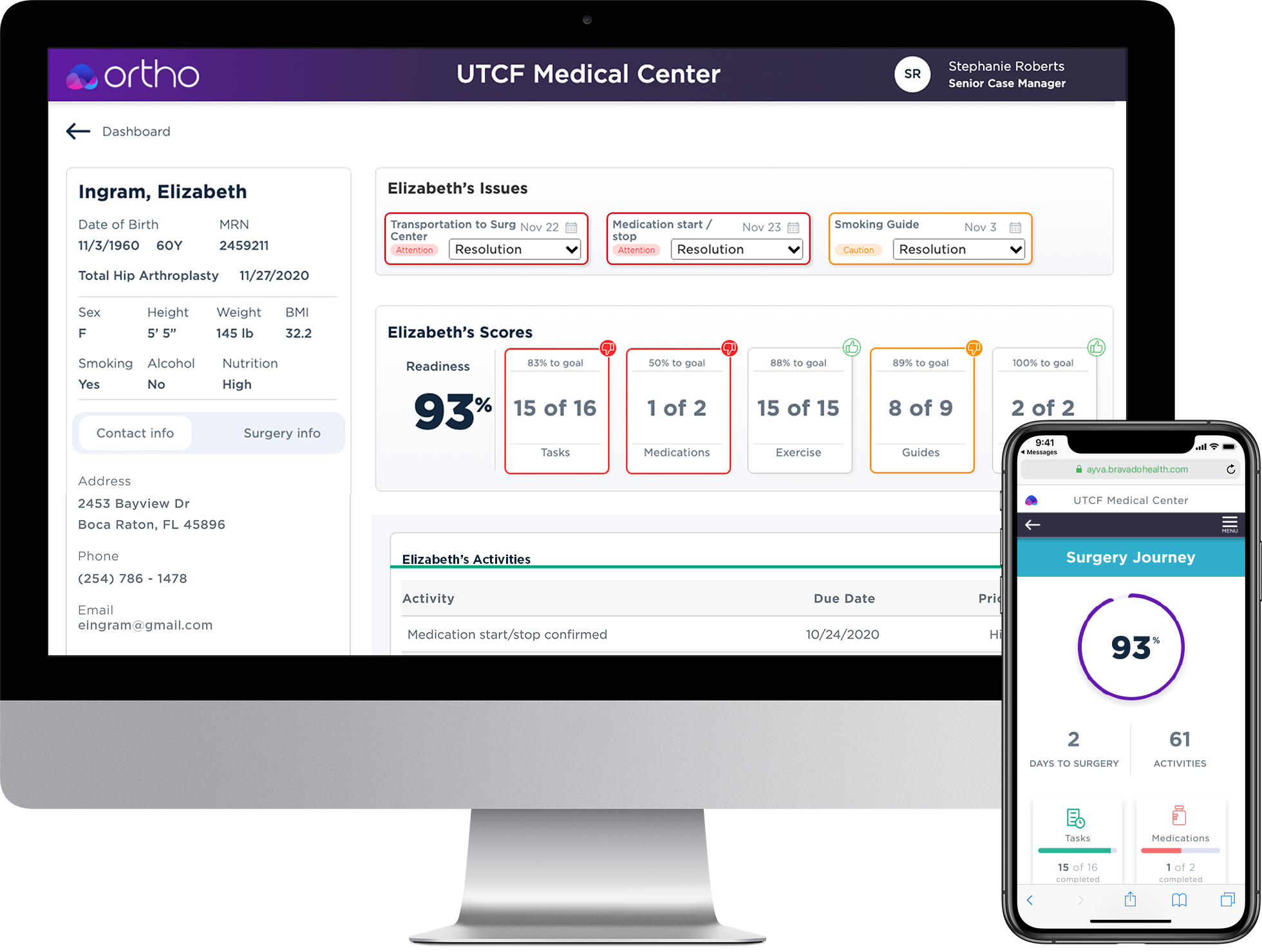
Built as an AI technology, Ayva automates communication between clinicians, case managers, and patients; while encouraging best practices for both pre-op preparedness and post-op recovery. Ayva Ortho (clinician-facing component) serves as an assistant for clinicians and case managers.
Overview
Ayva is a web-based application comprised of two interfaces, caregiver (clinician) and patient (mobile web).
Intended to:
- Improve the surgical journey for everyone involved
- Maximize case manager efficiency
- Improve outcomes
- Utilize evidence-based medicine as best practices
Ayva was born from strife, determination, and a realized need.
Why does Ayva Ortho work?
Nearly every physician, caregiver, and appointment scheduler has an app to manage patients. However, they rarely work the way a case manager might. For example, they do not show the right information at the right time or force the manager to click into a spreadsheet format. Instead, nearly every case manager uses Post-it notes or an electronic note application to do their job.
Ayva is different as it moves the case manager from being reactive, waiting until a patient fails or has questions. Instead, Ayva looks at where a patient is in their surgery journey and only alerts the case manager that there is something that they need to assist with.
I left Bravado Health before Ayva fully deployed, but the early data showed a marked improvement in how a case manager would balance their case loud. Antidotal comments, including, "We could never have managed Covid without Ayva," leave me optimistic.
Project roles and responsibilities
Product Design
Stakeholders
Applications
Myself leading two product designers and a UX writer. I was engineering liason.
Provide technical data on medical practices, guidelines for roadmap.
Axure (prototyping), Sketch and Zeplin transitioned into Figma.
Research, Interviews, Conceptions, Prototypes, and Final Design.
Chief Product Owner, Product Owner, Chief Medical Officer and Data Science
What is the Problem?
tive causes or because of an improved patient condition (1% each).
Today a significant loss, for hospitals and surgeons, is scheduled surgeries that don't take place. According to studies by the National Library of Medicine, 7 to 26% of surgeries are canceled depending on the hospital and type of surgery.
Patient no-shows were the most prevalent reason for surgical cancellation (63%). The second most common reason was surgical (17%), including changes in surgical plans. Acute conditions were the third most common cause (14%). Very few cancellations occurred due to administrative reasons or an improved patient condition (1% each).

63%
Patient no shows

17%
Surgical Issues

14%
Acute conditions
Why is this happening?
Surgery is scary, even when it's elective; even people who have had multiple surgeries report a sense of dread and helplessness. No wonder 16% of patients would rather face life-ending decisions than have surgery.
- Patients are not confident that they understand the surgical process.
- Patients' families and advocates may not believe the patient needs the surgery.
- Patients fear the pain during recovery and often question if they will ever be well again.
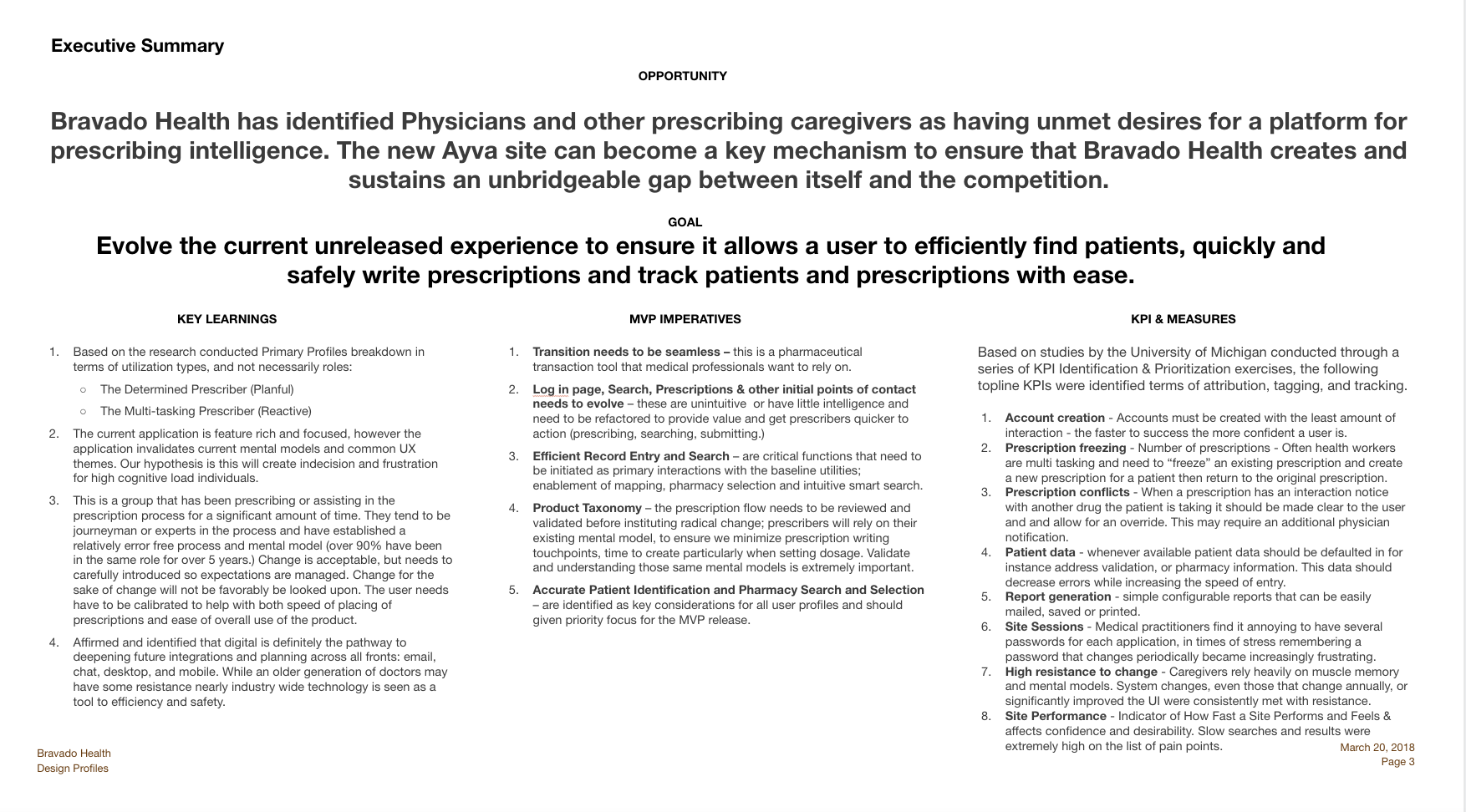
Solution
Create a system that allows surgeons and case managers to move from being reactive to proactive.
- Do away with having to look for information in multiple applications (spreadsheets, schedulers, and Post-its).
- Automate the reminders that go out to only the patients who need reminders.
- Encourage patients through education while allowing them to learn when convenient for them.
- Case managers quickly identify off-track patients.
- Case managers can visually see how to course correct when patients aren't following the surgery plan.
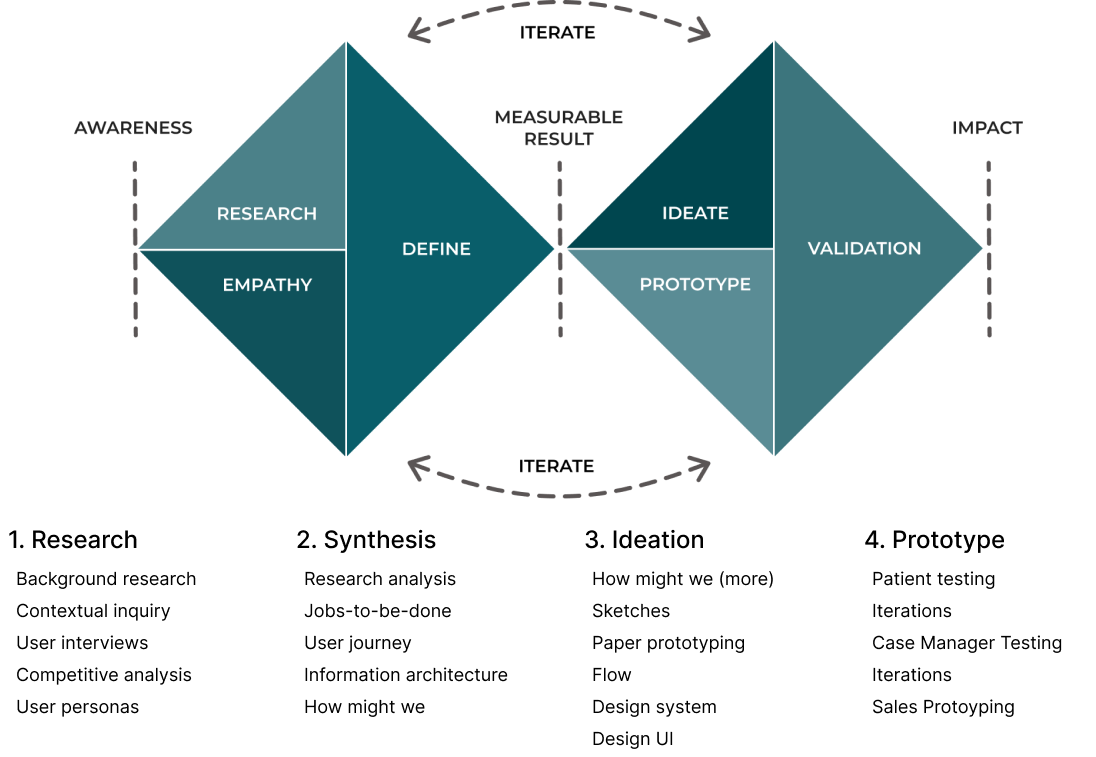
Design process
I chose Double Diamond. It's been around for 20 years. I knew this would be several years of changes as we learned and grew.
We needed a design process that evolved around research and iterations.
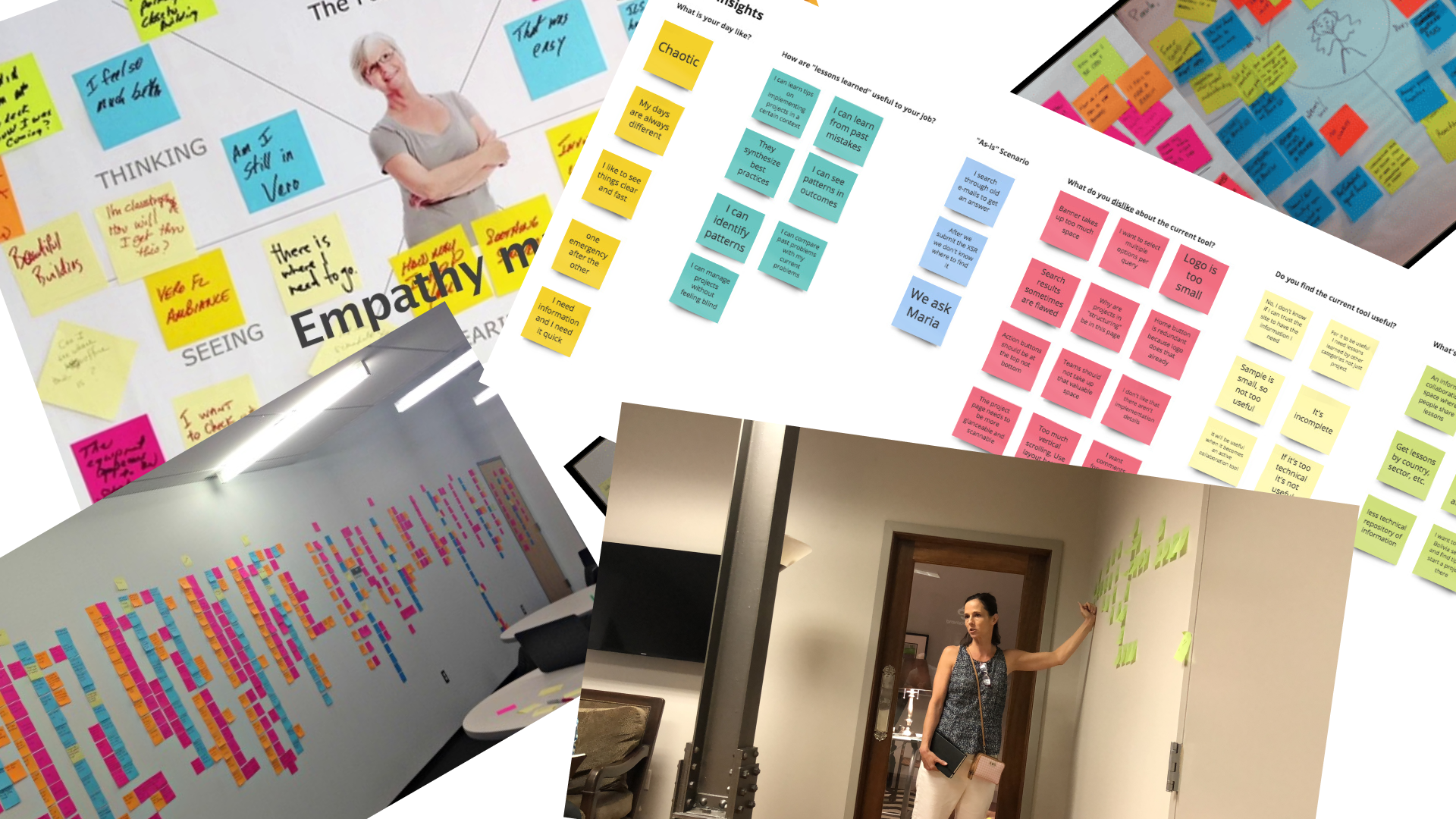
Research
Our user research uncovered clear pain points we needed to address with the application. For example, case managers work very hard, and during Covid, their workload increased significantly. Before Covid, a case manager might spend 15 to 30 minutes during the biweekly contact. During Covid, the time spent per patient increased from 45 minutes to an hour or more, and contact frequency increased to once or even twice a week in instances where the patient was at higher risk.
Pain Points
Patients have not arranged for payment or insurance coverage.
Patients have not made medication changes or followed Hibiclens protocol.
Patient social detriments were not uncovered prior to surgery.
Patient is not prepared for the recovery cycle. A patient may then allow the first two days after surgery to dictate the outcome.
Synthesis
Qualitative - With a medical application, more diligence is required when doing research. There is more data to review, and it has to be validated with the current advancements in the medical world.
Quantitive - We talked to industry experts, advisors, board members, and our staff SMEs. We also painstakingly detailed calls that case managers took and reviewed how they worked.
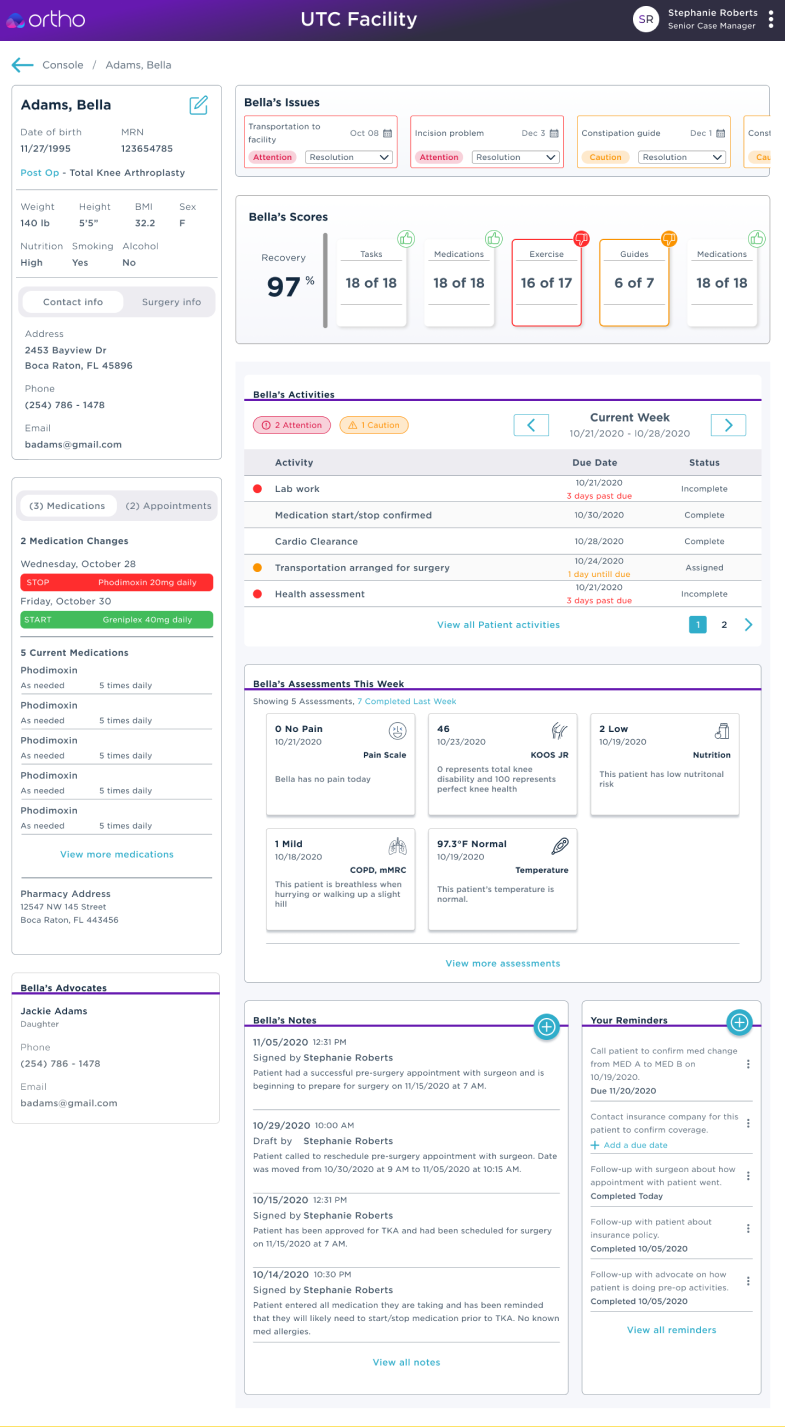
Ideation
Ideation took the form of working on "How might we..." statements, sketches, low and high-fidelity wireframes. We also started imagining the type of UI and controls. Would the practice need charts or tables? Could data be encapsulated in cards etc.? Early iterations focused on too much data. Several iterations later, we had just enough information visible to be efficient and detailed information easily accessible.
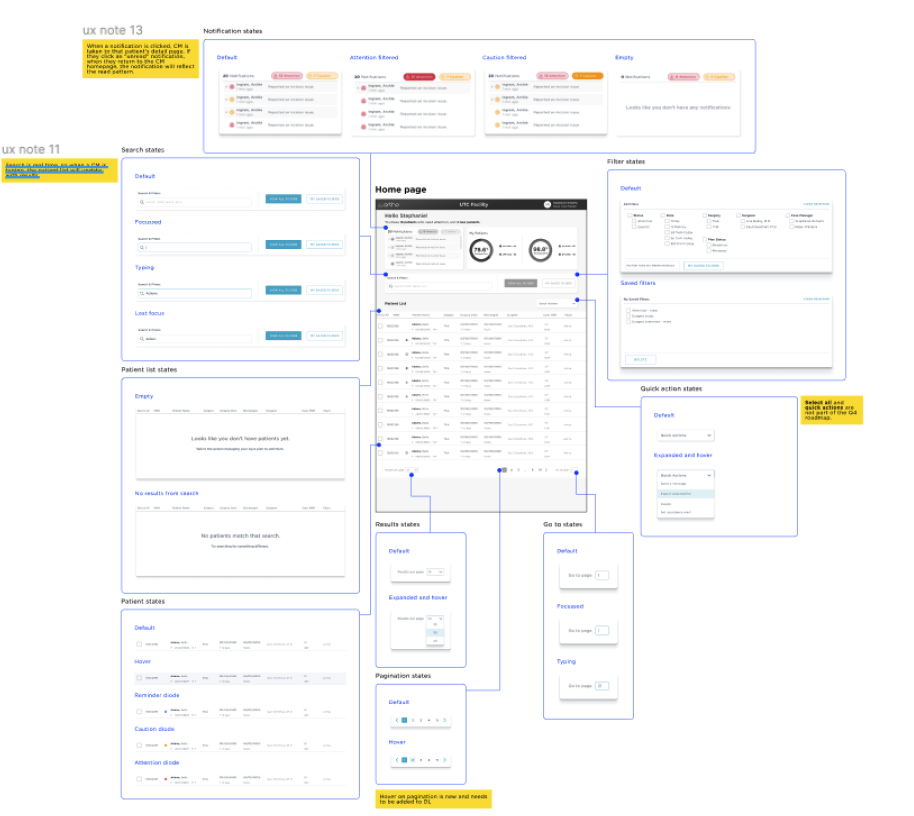
Wireframes
Over the next few weeks and several iterations, I fleshed out the white-boarded solutions in clickable prototypes across several viewport widths. While the software will be responsive, most users will mainly be on desktops, so I focused on that. I also tested tablet screens to ensure the designs could scale down. However, the use case wasn't as strong on mobile, and we decided to focus on 976px and up.
Prototyping

Paper prototyping works well, but during Covid, it proved to be very difficult to test with. Figma prototyping was fast, but the data was static and didn't reflect the interactions we needed to confirm. Axure excelled at this giving us the result we required.
Please feel free to review the Axure prototype V4. Great examples are:
Other examples may or may not work.
Conclusion
Due to brevity, I only shared a few of the many daily design decisions.
I worked with the team to manage issues:
- 8pt grid
- Design library management
- Design tokens
- Voice
- Content management
- HIPAA (and other regulations)
Click below to see the patient-facing mobile web case study.
Case Studies
Pearl - Case StudyProduct Design

Ayva Ortho - Case StudyProduct Design
Ayva (Patient Facing) - Case StudyProduct Design
© 2012-2023 James Young -- Principal Product Designer